
Pain often defies easy description for most individuals
Pain encompasses numerous sensations and emotional responses. Some experience it merely as an ache, while others endure a complex blend of aching, burning, occasional sharp sensations, muscular tension, tingling, or countless other manifestations.
Pain may have an identifiable cause (though not in all cases), consist of various contributing factors, and consequences that typically affect sleep quality, emotional wellbeing, and participation in cherished activities.
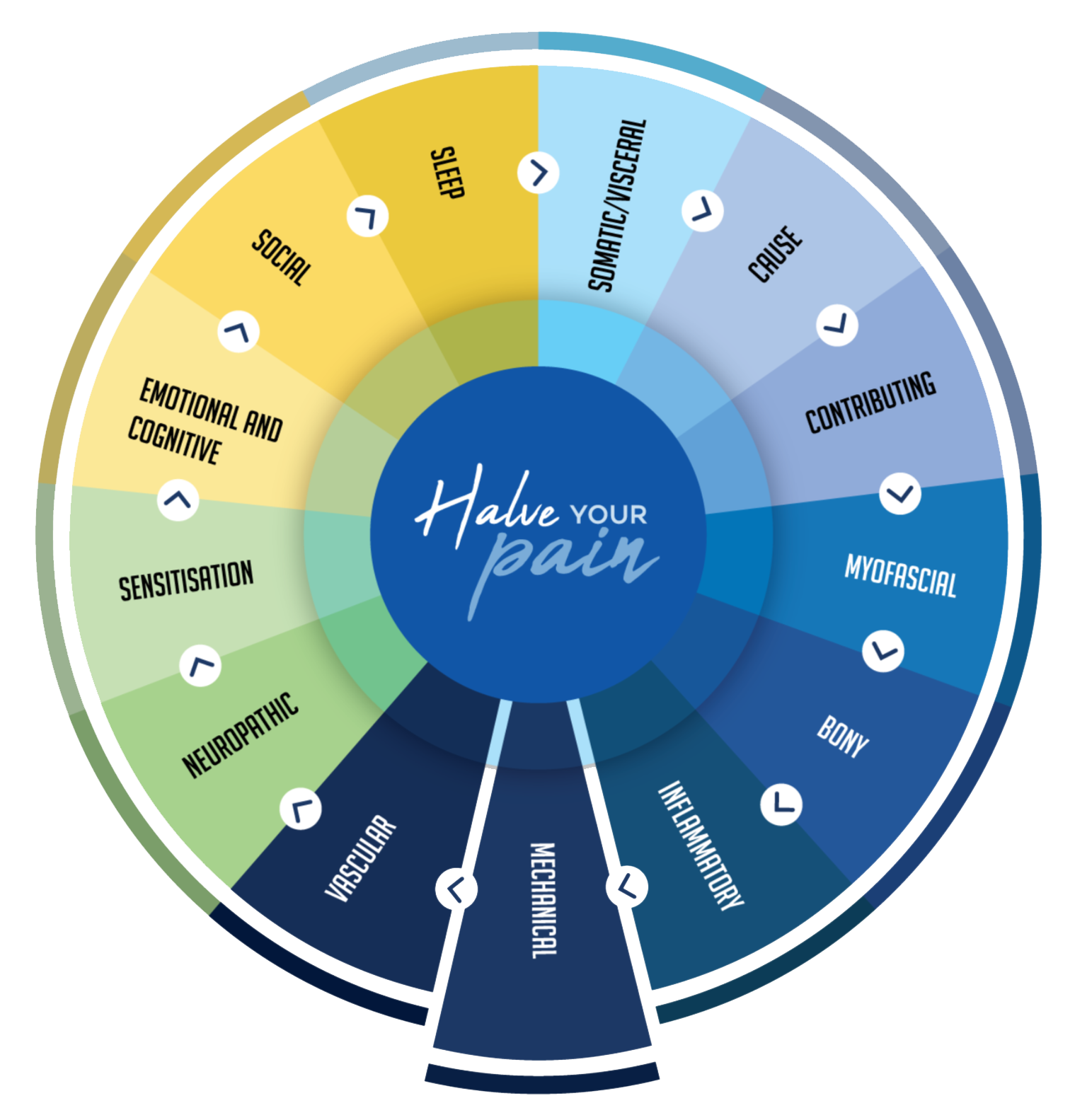
The Pain Pie offers a conceptual framework for understanding pain's complexity. It's not based on specific research, but rather serves as an explanatory tool illustrating that pain isn't a singular sensation. From a technical standpoint, the Pain Pie divides the pain system into three components, each represented by different colored segments. The blue sections represent pain originating from physical structures, green indicates nerve-generated pain, and yellow represents pain that emerges from or is intensified by the brain and spinal cord. Each segment features distinct characteristics and corresponding treatment approaches—some unique, others overlapping, as detailed below.
The Pain Pie also helps avoid the trap of seeking a single solution to pain management, such as "Surgery will completely fix your problem" or "You simply need to change your mindset about pain." While these approaches may be valuable components of treatment, they rarely provide substantial pain reduction when implemented in isolation. Furthermore, if these methods prove ineffective, additional options remain available. The Pain Pie helps identify all contributing factors to your pain. Rather than addressing just one element—like using anti-inflammatories for inflammatory pain, which might only reduce discomfort by 10-20%—treating all segments aims to diminish the entire pie, potentially achieving greater overall pain relief.
THE NATURE OF PAIN
Somatic/Visceral or Nociceptive Pain.
The term "soma" translates to "body" in medical vocabulary. When we discuss "somatic pain," we're referring to discomfort that stems from physical structures within your body. The crucial question patients and clinicians face is pinpointing exactly "Which structure?"
This category of pain takes many forms—it might feel heavy and persistent, sharp and intermittent, or present as a throbbing pressure. It doesn't always stay put either; somatic pain frequently radiates beyond its source, sometimes following predictable patterns but often traveling in ways that seem random or confusing.
Diagnosis becomes relatively straightforward when dealing with localized pain (imagine an area no larger than a golf ball). However, the detective work grows considerably more complex when pain spreads across expansive regions—picture an area the size of a football or larger. Don't lose heart though—clinical approaches exist to gradually narrow down these larger pain fields to identify their origins.

Causes of Pain

Pain origins can be either immediately apparent or frustratingly mysterious. Interestingly, in many patients, the initial injury has completely resolved, yet the pain persists independently. Even more confounding, pain signals may originate from unexpected sources. Take knee osteoarthritis, for instance—research shows approximately 32% of pain actually stems from structures outside the joint itself, explaining why treatments targeting only internal joint components may fail to provide relief.
When examining lower back pain, clinicians typically consider five primary culprits: facet joints, sacroiliac joints, hip structures, spinal discs, and nerve pathways. To navigate this complexity, healthcare providers employ a diagnostic strategy involving questions about pain triggers, precise location, radiation patterns, alleviating or aggravating factors, and accompanying symptoms. This investigative approach helps isolate the primary source of discomfort. The challenge lies in symptom overlap—many pain characteristics aren't exclusive to a single structure. Additionally, severe pain tends to create a generalized sensitivity where everything becomes painful, further complicating accurate diagnosis.
Contributing Factors
Contributing factors encompass a diverse range of physical conditions and attributes that can influence pain patterns. These include joint hypermobility (excessive range of motion), physical deconditioning (reduced fitness), muscle strength deficiencies, body weight considerations, and joint alignment issues. Core stability—the functional strength of muscles supporting your spine and pelvis—also plays a significant role in this category. Successfully identifying these underlying contributors and implementing appropriate interventions represents a crucial component of developing an effective pain management strategy.
Myofascial Pain
Muscle tension and trigger points constitute the key myofascial components in pain conditions. These trigger points—often overlooked in pain assessment—can generate both concentrated discomfort and referred pain that travels extensively, often masquerading as nerve-based or structural pain patterns.
When addressing myofascial discomfort, techniques like manipulation, acupuncture or massage therapy typically provide only short-term benefits—usually lasting between 24-72 hours. This happens because muscle tension frequently develops as a secondary reaction to primary issues elsewhere. Consider how problems with the facet joints in spinal regions frequently trigger protective muscular contractions in surrounding tissues.
Interestingly, weakness can paradoxically present as tightness in muscular systems. Picture this scenario: despite lacking adequate strength, muscles must still perform their functional roles (supporting your posture, for example). The body compensates for this weakness by maintaining constant tension—essentially working overtime. In these cases, focusing exclusively on releasing tension proves insufficient; implementing progressive strengthening protocols becomes the cornerstone of effective treatment.

Bony Pain.
Impact-related discomfort characterizes what we might term "osseous pain"—a condition that manifests when pressure is applied to affected structures (standing up triggers pain, while sitting relieves it), when direct pressure is applied over bone surfaces, or when discomfort disrupts sleep patterns. Identifying this pain category presents particular challenges in spinal regions but becomes more readily apparent in peripheral joints and extremities like knees, legs, and feet.
Management approaches for bone-related pain mirror fracture treatment protocols—primarily focusing on load reduction to allow natural healing processes to progress. Emerging research has also demonstrated the effectiveness of bisphosphonate medications (typically prescribed for osteoporosis) in alleviating bone pain associated with osteoarthritic conditions.

Inflammatory Pain
Pain with inflammatory origins follows distinctive patterns—typically worse upon waking and after periods of inactivity. Key characteristics include morning stiffness, visible swelling, improvement with heat application, worsening with cold exposure, and temporary response to anti-inflammatory medications. This pain category often disrupts sleep initiation or causes nighttime awakening, and many patients report weather-related symptom fluctuations (your knee might literally forecast approaching rain).
Most chronic pain conditions contain an inflammatory component. In osteoarthritis, morning stiffness typically resolves within 5-60 minutes as movement increases. However, when stiffness persists beyond 30-60 minutes, or when stiffness rather than pain represents your primary complaint, these patterns suggest possible inflammatory arthritis conditions like rheumatoid arthritis. Such indicators warrant medical consultation and potential rheumatology referral, particularly given the expanding range of effective therapeutic options now available for these conditions.
MECHANICAL PAIN
The term "mechanical pain" encompasses various manifestations rather than fitting a single description. While commonly defined as discomfort triggered by specific movements or postures and relieved when that action ceases, I find this characterization somewhat limiting.
A more useful approach considers the broader "mechanical features" of pain—including painful clicking/clunking sensations, instances of joint instability or "giving way," locking episodes, and restricted motion range. The underlying cause varies depending on which body structure is involved. Though these mechanical symptoms might suggest surgical intervention, this isn't universally necessary.
Take ACL (anterior cruciate ligament) tears as an example: while surgical repair is standard practice in Australia, research from Scandinavia reveals that approximately half of patients may not actually require surgery. Their studies demonstrate that with comprehensive rehabilitation, non-surgical patients often achieve comparable activity levels to those who undergo surgical intervention.

Vascular Pain.
Vascular or ischemic pain develops when blood supply to tissues becomes insufficient. Though less common in spinal and extremity pain conditions, it's frequently observed in individuals with peripheral vascular disease. This pain mechanism involves inadequate blood delivery to working muscles—as muscles increase activity, the compromised circulation cannot meet oxygen demands, resulting in pain. This pattern typically affects calf or thigh muscles, with uphill walking or stair climbing being classic triggers. A key diagnostic feature is rapid pain resolution once activity stops.
The management approach begins with accurate diagnosis and locating the specific vascular blockage point. Treatment strategy depends on underlying causes and may include:
Controlling cardiovascular risk factors like hypertension and elevated cholesterol
Smoking cessation
Optimizing diabetes management
Implementing structured exercise programs, which have demonstrated effectiveness for this pain type
When conservative measures prove insufficient, interventional options include angioplasty or stent placement to widen narrowed vessels. In cases where muscular bands compress blood vessels, Botox injections can provide relief. As a final resort, surgical bypass procedures may be necessary to circumvent persistent blockages.
Neuropathic Pain.

Nerve damage or disease produces neuropathic pain, though many patients display "neuropathic features" without actual nerve injury. A common example is shoulder pain accompanied by occasional hand tingling—likely stemming from nerve irritation rather than damage.
Neuropathic characteristics include burning sensations, tingling, numbness, electric shock sensations, itching, crawling feelings (formication), pain from light touch (allodynia), painful cold, and squeezing sensations. These symptoms often appear randomly without clear patterns. This pain type frequently seems disproportionately severe (hyperalgesia) and causes significant emotional distress.
Treatment typically involves medication and neurostimulation. Common medications include amitriptyline (Endep), pregabalin (Lyrica), and duloxetine (Cymbalta/Andepra)—which despite being classified as antidepressants or anti-epileptics, function as nerve stabilizers by restoring normal pain inhibition. Side effects are numerous, with drowsiness being most common. This can be managed through low initial dosing with gradual increases. Since metabolism varies between individuals, switching medications may help when side effects occur. Topical application as creams can reduce systemic absorption and minimize side effects. Medications should be trialed for 4-6 weeks before determining effectiveness.
Neurostimulation delivers electrical pulses to alter nerve function and reduce pain through implanted leads connected to a subcutaneous battery. Options include PENS (60-minute stimulation providing 6-12 months relief), permanent peripheral nerve stimulation (effective for headaches, chest wall, and focal buttock pain), spinal cord stimulation for back and leg pain, and dorsal root ganglion stimulation for focused nerve pain.

Sensitisation

Sensitisation can be thought of as amplification of the pain. Key indicators are: Severe pain out of proportion to the injury (eg little injury but big pain). Pain that is unpredictable, always there, spreads or moves, has multiple things that trigger it off, is associated anxiety or depression and social issues, such as job loss, financial stress or relationship issues.
Sensitisation can be pictured as the ‘volume control’ for your pain. Commonly, pain is ‘turned down’ (eg it is silent), particularly from degenerative problems, which normally don’t cause pain. But changes occur in the nervous system resulting in the volume being ‘turned up’, and “Things that shouldn’t hurt, do hurt, and things that should only hurt a little bit, hurt a lot”.
For the fortunate few, pain remains a purely physical experience that doesn't interfere with daily functioning or emotional wellbeing—these rare individuals simply push through without significant impact.
Most people, however, experience natural emotional responses to persistent pain—feelings of lowered mood and heightened vigilance or worry about activities that might worsen their discomfort. When these responses intensify and begin disrupting everyday functioning, they may be classified as depression and anxiety. The frustrating reality is that these emotional states can then amplify pain perception, creating an unfair, self-perpetuating cycle.
A crucial breakthrough comes with recognizing that depression and anxiety often develop as responses to pain—not character flaws or signs of personal weakness. This understanding opens the door to addressing these emotional components through psychological support, mindfulness practices, physical activity, or appropriate medications. Treating these emotional dimensions becomes another valuable strategy in your comprehensive pain management approach.
